Newsletter
Issue 2 Summer 2005

|
Newsletter |
|
|
Injury - more attention
to the world’s neglected epidemic?
|
|
In the developing world infectious disease grabs all the headlines, in the developed world cancer and heart disease are always in the news. However, there is now a growing interest from politicians and health planners in trauma as a global health problem. The strong leadership from the WHO Department for Injuries and Violence Prevention http://www.who.int/violence_injury_prevention/en/ has made a major contribution to this mind shift. |
|
|
Appropriately, injury prevention is a major focus of the work of the WHO department but the strong WHO support for the CRASH-2 trial signals very clearly that trauma care is also high up on the agenda. Importantly, the recent publication by WHO ‘Guidelines for Essential Trauma Care’ offers a blueprint for an effective trauma system that is applicable across the world, whatever a country’s state of economic development. The global approach to the epidemic of injury fits very well with the global approach of the CRASH-2 trial – leading on from the original CRASH trial we are very much at the forefront of moulding the way that clinicians, and perhaps also politicians, think about injury. In the past coagulation following injury has been seen as problem that occurs several hours after injury. A coagulation screen was not included in the ATLS list of blood tests until the latest edition. It is now known that many patients have disturbed coagulation on arrival in the Emergency Room, and that this is an independent risk factor for death. Modulation of clot breakdown by an antifibrinolytic has the potential to improve patient outcomes by preventing bleeding (the cause of half of in-hospital deaths following injury). The publicity around recombinant factor VIIa has added to the enthusiasm for non-surgical methods of bleeding control following trauma. The combination of a growing political awareness of the importance of trauma to the World Burden of Disease and the growing clinical awareness of the importance of non-surgical approaches to bleeding control following injury means that everyone involved in the CRASH-2 trial is right at the cutting edge of current thinking about trauma management. Tim Coats |
|
| CRASH-2
TRIAL OFFICIALLY LAUNCHED We used the opportunity of the CRASH Trial close-out meeting which was held in April at St Catherine's College, Oxford, to officially launch the CRASH-2 Trial. Collaborators representing 27 countries attended. The most important outcome of the meeting was the shared desire to maintain this fantastic collaborative group and to expand it even more. |
|
 |
|
recruitment has
started!!! |
|
|
Hospitals in 5 countries have started recruiting patients:
* * * CONGRATULATIONS * * *
|
|
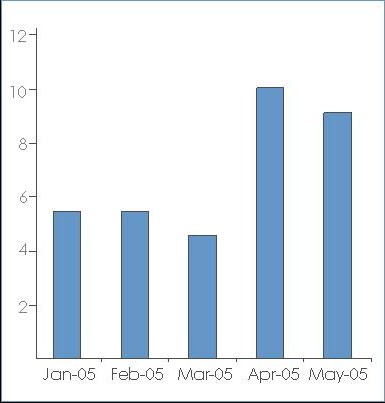
ETHICS APPROVALS PER MONTH 43 hospitals already
have
Many
congratulations |
 |
 |
ALBANIA - Fatos Olldashi, National Trauma Centre Hospital |
 |
ARGENTINA
- Fernanda Barboza, Hospital Dr Ramón Carrillo - Gustavo Pinero, Hospital Municipal "Dr Leonidas Lucero" - Karina Surt, Hospital Escuela Jose de San Martin |
 |
BELGIUM - Guy Mazairac, Centre Hospitalier Regional de Namur |
 |
COLOMBIA - Juan Diego Ciro Quintero, Clinica Las Americas - Jorge H Mejia-Mantilla, Fundacion Clinica Valle del Lili - Hernándo Delgado Chaves, Hospital Civil De Ipiales |
 |
CUBA - Nelvio Durán Rodríguez, Hospital General Docente "Dr Agostinho Neto" - Irene Zamalea Bess, Hospital Miguel Enriquez - Aida Madrazo Carnero, Hospital Provincial Docente V.I. Lenin - Ernesto Miguel Piferrer Ruiz, Hospital Clínico-Quirúrgico Docente Saturnino Lora" |
 |
ECUADOR - Mario Izurieta Ulloa, Hospital Luis Vernaza - Inés Zavala, Hospital de Niños Dr. Roberto Gilbert Elizalde |
 |
EGYPT - Mamdouh Alamin, Aswan Teaching Hospital - Hussein Khamis, Mataria Teaching Hospital - Hesham El-Sayed, Suez Canal University |
 |
GEORGIA - Tamar Gogichaisvili, Tbilisi State Medical University |
 |
INDIA - Rajesh Bhagchandani, Apex Hospital Bhopal - Sanjay Gupta, Sri Sai Hospital - Y R Yadav, NSCB Medical College - Vijaya Ushanath Sethurayar, Meenakshi Mission Hospital & Research Centre - Yashbir Dewan, Christian Medical College - Wu Hoong Chhang, North Bengal Neuro Research Centre - Mazhar Husain, King George's Medical University - Ashok Kumar Mahapatra, All India Institute of Medical Sciences (AIIMS) - Anup K Saha, Burdwan Medical College Hospital - Haroon M Pillay, Baby Memorial Hospital |
 |
INDONESIA
- Moch Dwikoryanto, Soebandi Hospital Jember - Nyoman Golden, Sanglah General Hospital |
 |
NIGERIA - Edward O Komolafe, Obafemi Awolowo University Teaching Hospitals - B B Shehu, Usmanu Danfodiyo University Teaching Hospital - Olugbenga Oludiran, University of Benin Teaching Hospital - Kehinde S Oluwadiya, LAUTECH Teaching Hospital |
 |
TUNISIA - Zouheir Jerbi, Hospital Habib Thameur |
 |
UK - Jay Banerjee, Leicester Royal Infirmary |
|
most frequently asked questions 'RISK OF SIGNIFICANT
HAEMORRHAGE'
TRAUMA SCORING SYSTEM? Physiological severity
scores, such as the Revised Trauma Score, give a heavy weight to level
of consciousness, so they do not define the group that has significant
bleeding. All forms of scoring require training and add a level of complexity
to the patient entry process. For these reasons a severity score has not
been used in the CRASH-2 trial. |
